Human development/Description: Difference between revisions
Jump to navigation
Jump to search
m (Text replace - "FormulaTemplate" to "FormulaAndTableTemplate") |
No edit summary |
||
| Line 11: | Line 11: | ||
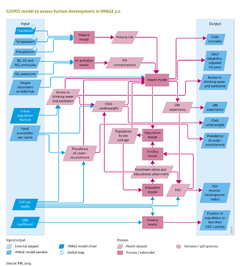
The risk-factor-attributable component is based on a multi-state approach, distinguishing exposure, disease and death ([[WHO, 2002]];[[Cairncross and Valdmanis, 2006]]). This implies that for various health-risk factors, incidence and case fatality rates (i.e. the ratio of the number of deaths caused by a specific disease over the number of diagnosed cases) are taken into account. The level of health services modifies case fatality rates. This methodology is used for malaria, diarrhoea and pneumonia; the approach for protein deficiency is discussed below. The method for projecting mortality due to other causes of death (non-communicable chronic diseases, other communicable diseases and injuries) follows the global burden of disease ([[HasAcronym::GBD]]) approach that uses a parsimonious regression technique to related mortality rates of 10 major disease clusters with GDP, smoking behaviour and human capital ([[Mathers and Loncar, 2006]]). This methodology is used for the causes of death related to urban air pollution. | The risk-factor-attributable component is based on a multi-state approach, distinguishing exposure, disease and death ([[WHO, 2002]];[[Cairncross and Valdmanis, 2006]]). This implies that for various health-risk factors, incidence and case fatality rates (i.e. the ratio of the number of deaths caused by a specific disease over the number of diagnosed cases) are taken into account. The level of health services modifies case fatality rates. This methodology is used for malaria, diarrhoea and pneumonia; the approach for protein deficiency is discussed below. The method for projecting mortality due to other causes of death (non-communicable chronic diseases, other communicable diseases and injuries) follows the global burden of disease ([[HasAcronym::GBD]]) approach that uses a parsimonious regression technique to related mortality rates of 10 major disease clusters with GDP, smoking behaviour and human capital ([[Mathers and Loncar, 2006]]). This methodology is used for the causes of death related to urban air pollution. | ||
The GISMO health model considers mortality due to | The GISMO health model considers mortality due to | ||
# Malaria; | |||
# Communicable and infectious diseases associated with undernourishment, poor access to safe drinking water and basic sanitation and poor indoor air quality; | |||
# Diseases caused by poor outdoor air quality; | |||
# HIV-AIDS; | |||
# Chronic diseases including high blood pressure and obesity. | |||
Here, we only discuss the first three causes of mortality as they are linked to environmental factors. The mortality rate due to a specific disease is a multiplication of the incidence rate (fraction of the population with the specific disease) and the case fatality rate (the fraction of people who die from a specific disease), distinguishing for the two sexes and five-year age cohorts. These mortality rates can then be used to calculated age-specific life expectancy (for details see [[Hilderink, 2000]]). | |||
(i) Malaria risk. In the [[GISMO model]], incidence rates of malaria are determined by the areas which are suitable for the malaria mosquito, based on the monthly climatic factors of temperature and precipitation ([[Craig et al., 1999]]). Incidence rates are decreased by the level of insecticide treated bed nets and indoor residual spraying, modelled separately as potential policy options. The case fatality rate of malaria is increased by underweight levels and decreased by case management, i.e. treatment. | (i) Malaria risk. In the [[GISMO model]], incidence rates of malaria are determined by the areas which are suitable for the malaria mosquito, based on the monthly climatic factors of temperature and precipitation ([[Craig et al., 1999]]). Incidence rates are decreased by the level of insecticide treated bed nets and indoor residual spraying, modelled separately as potential policy options. The case fatality rate of malaria is increased by underweight levels and decreased by case management, i.e. treatment. | ||
Revision as of 13:41, 16 December 2013
Parts of Human development/Description
| Component is implemented in: |
|
| Related IMAGE components |
| Projects/Applications |
| Models/Databases |
| Key publications |
| References |
{kind=link}