Human development/Description: Difference between revisions
Jump to navigation
Jump to search
No edit summary |
No edit summary |
||
| Line 2: | Line 2: | ||
|Status=On hold | |Status=On hold | ||
|Reference=Hilderink, 2000; UNDP, 1990; UNDP, 2010; WHO, 2002; Cairncross and Valdmanis, 2006; Mathers and Loncar, 2006; Craig et al., 1999; Smith and Haddad, 2000; De Onis and Blossner, 2003; FAO, 2003; Mathers and Loncar, 2006; Pandey et al., 2006; Dockery et al., 1993; Pope et al., 1995; Ravallion et al., 2008; | |Reference=Hilderink, 2000; UNDP, 1990; UNDP, 2010; WHO, 2002; Cairncross and Valdmanis, 2006; Mathers and Loncar, 2006; Craig et al., 1999; Smith and Haddad, 2000; De Onis and Blossner, 2003; FAO, 2003; Mathers and Loncar, 2006; Pandey et al., 2006; Dockery et al., 1993; Pope et al., 1995; Ravallion et al., 2008; | ||
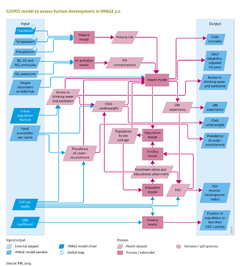
|Description=In the GISMO model, the impacts of global environmental change on human development are modelled by considering impacts on human health – either directly, for example, via the impact of climate change on malaria, or indirectly, such as by the impact of climate change on food availability. In addition to environmental factors, human health is also driven by socioeconomic factors, including income levels and educational attainment. To take account of these different factors and their interrelation, the GISMO model consists of three modules that address human health, poverty and education (see Figure on the right). The modules are linked through a cohort component population model, including endogenous fertility and mortality (for details see [[Hilderink, 2000]]). Fertility levels are modelled using a convergence level that is determined by female educational levels, and a speed of convergence, determined by the human development index ([[HDI]]) (see below). Mortality rates are determined by the health module, which is discussed in further detail in the remainder of this section. Future trends in migration, including urbanisation, are put exogenously into the model (for details see [[Hilderink, 2000]]) | |Description=== Description == | ||
In the GISMO model, the impacts of global environmental change on human development are modelled by considering impacts on human health – either directly, for example, via the impact of climate change on malaria, or indirectly, such as by the impact of climate change on food availability. In addition to environmental factors, human health is also driven by socioeconomic factors, including income levels and educational attainment. To take account of these different factors and their interrelation, the GISMO model consists of three modules that address human health, poverty and education (see Figure on the right). The modules are linked through a cohort component population model, including endogenous fertility and mortality (for details see [[Hilderink, 2000]]). Fertility levels are modelled using a convergence level that is determined by female educational levels, and a speed of convergence, determined by the human development index ([[HDI]]) (see below). Mortality rates are determined by the health module, which is discussed in further detail in the remainder of this section. Future trends in migration, including urbanisation, are put exogenously into the model (for details see [[Hilderink, 2000]]) | |||
The Human Development Index (HDI), introduced in the UNDP Human Development Report 1990, to rank development achievement is a composite index of life expectancy, education, and income indices ([[UNDP, 1990]];[[UNDP, 2010]]). The underlying indicators have been refined several times, over the years, while the three elements have remained the same. The index links to the three GISMO model components. | The Human Development Index (HDI), introduced in the UNDP Human Development Report 1990, to rank development achievement is a composite index of life expectancy, education, and income indices ([[UNDP, 1990]];[[UNDP, 2010]]). The underlying indicators have been refined several times, over the years, while the three elements have remained the same. The index links to the three GISMO model components. | ||
| Line 18: | Line 19: | ||
# Chronic diseases including high blood pressure and obesity. | # Chronic diseases including high blood pressure and obesity. | ||
Here, we only discuss the first three causes of mortality as they are linked to environmental factors. The mortality rate due to a specific disease is a multiplication of the incidence rate (fraction of the population with the specific disease) and the case fatality rate (the fraction of people who die from a specific disease), distinguishing for the two sexes and five-year age cohorts. These mortality rates can then be used to calculated age-specific life expectancy (for details see [[Hilderink, 2000]]). | Here, we only discuss the first three causes of mortality as they are linked to environmental factors (see Table). The mortality rate due to a specific disease is a multiplication of the incidence rate (fraction of the population with the specific disease) and the case fatality rate (the fraction of people who die from a specific disease), distinguishing for the two sexes and five-year age cohorts. These mortality rates can then be used to calculated age-specific life expectancy (for details see [[Hilderink, 2000]]). | ||
{{FormulaAndTableTemplate|Table_HD}} | |||
=== Malaria risk === | === Malaria risk === | ||
| Line 30: | Line 33: | ||
Trends in access to modern energy sources are taken from the TIMER residential [[Energy demand]] model. | Trends in access to modern energy sources are taken from the TIMER residential [[Energy demand]] model. | ||
Child underweight and prevalence of undernourishment. For children under the age of five, undernourishment is expressed as underweight (measured as weight-for-age), whereas for older ages prevalence of undernourishment is used. The direct effect of undernourishment is protein deficiency, which for children mortality rates is scaled to their underweight status; for older age groups, mortality rates are scaled to levels of undernourishment. Indirectly, undernourishment increases the incidence of diarrhoea and pneumonia, and the case fatality of malaria, diarrhoea and pneumonia. These indirect effects are only modelled for children under the age of five. | Child underweight and prevalence of undernourishment. For children under the age of five, undernourishment is expressed as underweight (measured as weight-for-age), whereas for older ages prevalence of undernourishment is used. The direct effect of undernourishment is protein deficiency, which for children mortality rates is scaled to their underweight status; for older age groups, mortality rates are scaled to levels of undernourishment. Indirectly, undernourishment increases the incidence of diarrhoea and pneumonia, and the case fatality of malaria, diarrhoea and pneumonia. These indirect effects are only modelled for children under the age of five. | ||
Revision as of 19:29, 16 December 2013
Parts of Human development/Description
| Component is implemented in: |
|
| Related IMAGE components |
| Projects/Applications |
| Models/Databases |
| Key publications |
| References |
{kind=link}