Human development/Description: Difference between revisions
Jump to navigation
Jump to search
No edit summary |
No edit summary |
||
| Line 50: | Line 50: | ||
Only the first three causes of mortality are considered because these are linked to environmental factors. The mortality rate due to a specific disease is a multiplication of the incidence rate (fraction of the population with the specific disease) and the case fatality rate (the fraction of people who die from a specific disease), distinguishing for the two sexes and five-year age cohorts. These mortality rates can then be used to calculated age-specific life expectancy (for details see [[Hilderink, 2000]]). | Only the first three causes of mortality are considered because these are linked to environmental factors. The mortality rate due to a specific disease is a multiplication of the incidence rate (fraction of the population with the specific disease) and the case fatality rate (the fraction of people who die from a specific disease), distinguishing for the two sexes and five-year age cohorts. These mortality rates can then be used to calculated age-specific life expectancy (for details see [[Hilderink, 2000]]). | ||
====Malaria risk=== = | ====Malaria risk==== | ||
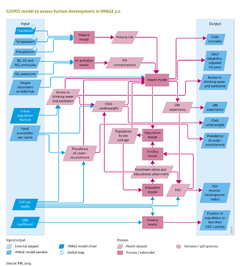
Incidence rates of malaria are determined by the areas suitable for the malaria mosquito, based on monthly temperature and precipitation, see Component [[Water]] ([[Craig et al., 1999]]). Incidence rates are decreased by the level of insecticide treated bed nets and indoor residual spraying, modelled separately as potential policy options. The case fatality rate of malaria is increased by level of underweight people and decreased by case management (treatment). | Incidence rates of malaria are determined by the areas suitable for the malaria mosquito, based on monthly temperature and precipitation, see Component [[Water]] ([[Craig et al., 1999]]). Incidence rates are decreased by the level of insecticide treated bed nets and indoor residual spraying, modelled separately as potential policy options. The case fatality rate of malaria is increased by level of underweight people and decreased by case management (treatment). | ||
| Line 71: | Line 71: | ||
The education module assesses future developments in school enrolment and educational attainment, including literacy rates at three levels of education: primary, secondary and tertiary. The model tracks the proportion of the highest level of education completed and the average number of years of schooling per cohort. The enrolment ratios per educational level are determined using cross-sectional relationships with per-capita GDP (PPP). The age at which a certain educational level is attained is assumed to be identical in all regions. Literacy rates are determined by the proportion of the population over the age of 15 who have completed at least primary education. Furthermore, to take account of autonomous increases in literacy levels, literacy levels of the population between the age of 15 and 65 is increased by 0.3%, annually. | The education module assesses future developments in school enrolment and educational attainment, including literacy rates at three levels of education: primary, secondary and tertiary. The model tracks the proportion of the highest level of education completed and the average number of years of schooling per cohort. The enrolment ratios per educational level are determined using cross-sectional relationships with per-capita GDP (PPP). The age at which a certain educational level is attained is assumed to be identical in all regions. Literacy rates are determined by the proportion of the population over the age of 15 who have completed at least primary education. Furthermore, to take account of autonomous increases in literacy levels, literacy levels of the population between the age of 15 and 65 is increased by 0.3%, annually. | ||
}} | }} | ||
Revision as of 08:54, 20 May 2014
Parts of Human development/Description
| Component is implemented in: |
|
| Related IMAGE components |
| Projects/Applications |
| Models/Databases |
| Key publications |
| References |
{kind=link}