Human development/Description: Difference between revisions
Jump to navigation
Jump to search
No edit summary |
No edit summary |
||
| Line 1: | Line 1: | ||
{{ComponentDescriptionTemplate | {{ComponentDescriptionTemplate | ||
|Status=On hold | |Status=On hold | ||
|Reference=Hilderink, 2000; UNDP, 1990; UNDP, 2010; WHO, 2002; Cairncross and Valdmanis, 2006; Mathers and Loncar, 2006; Craig et al., 1999; | |Reference=Hilderink, 2000; UNDP, 1990; UNDP, 2010; WHO, 2002; Cairncross and Valdmanis, 2006; Mathers and Loncar, 2006; Craig et al., 1999; Smith and Haddad, 2000; De Onis and Blossner, 2003; FAO, 2003; Mathers and Loncar, 2006; Pandey et al., 2006; Dockery et al., 1993; Pope et al., 1995; Ravallion et al., 2008; | ||
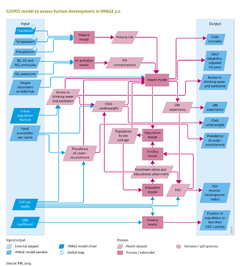
|Description=In the GISMO model, the impacts of global environmental change on human development are modelled by considering impacts on human health – either directly, for example, via the impact of climate change on malaria, or indirectly, such as by the impact of climate change on food availability. In addition to environmental factors, human health is also driven by socioeconomic factors, including income levels and educational attainment. To take account of these different factors and their interrelation, the GISMO model consists of three modules that address human health, poverty and education (Figure | |Description=In the GISMO model, the impacts of global environmental change on human development are modelled by considering impacts on human health – either directly, for example, via the impact of climate change on malaria, or indirectly, such as by the impact of climate change on food availability. In addition to environmental factors, human health is also driven by socioeconomic factors, including income levels and educational attainment. To take account of these different factors and their interrelation, the GISMO model consists of three modules that address human health, poverty and education (see Figure on the right). The modules are linked through a cohort component population model, including endogenous fertility and mortality (for details see [[Hilderink, 2000]]). Fertility levels are modelled using a convergence level that is determined by female educational levels, and a speed of convergence, determined by the human development index (HDI) (see below). Mortality rates are determined by the health module, which is discussed in further detail in the remainder of this section. Future trends in migration, including urbanisation, are put exogenously into the model (for details see [[Hilderink, 2000]]) | ||
The Human Development Index (HDI), introduced in the UNDP Human Development Report 1990, to rank development achievement is a composite index of life expectancy, education, and income indices ([[UNDP, 1990]];[[UNDP, 2010]]). The underlying indicators have been refined several times, over the years, while the three elements have remained the same. The index links to the three GISMO model components. | The Human Development Index (HDI), introduced in the UNDP Human Development Report 1990, to rank development achievement is a composite index of life expectancy, education, and income indices ([[UNDP, 1990]];[[UNDP, 2010]]). The underlying indicators have been refined several times, over the years, while the three elements have remained the same. The index links to the three GISMO model components. | ||
| Line 9: | Line 9: | ||
The GISMO health model describes the causal chains between health-risk factors and health outcomes, (morbidity and mortality) taking into account the effect of health services. The mortality rate is modelled through a risk-factor-attributable component and a non-attributable component. Historically, the non-attributable component represents the remainder of mortality not covered by the risk-factors included. For future projections, this component is assumed to reduce by the regional average historical rates of reduction. | The GISMO health model describes the causal chains between health-risk factors and health outcomes, (morbidity and mortality) taking into account the effect of health services. The mortality rate is modelled through a risk-factor-attributable component and a non-attributable component. Historically, the non-attributable component represents the remainder of mortality not covered by the risk-factors included. For future projections, this component is assumed to reduce by the regional average historical rates of reduction. | ||
The risk-factor-attributable component is based on a multi-state approach, distinguishing exposure, disease and death ([[WHO, 2002]];[[Cairncross and Valdmanis, 2006]]). This implies that for various health-risk factors, incidence and case fatality rates (i.e. the ratio of the number of deaths caused by a specific disease over the number of diagnosed cases) are taken into account. The level of health services modifies case fatality rates. This methodology is used for malaria, diarrhoea and pneumonia; the approach for protein deficiency is discussed below. The method for projecting mortality due to other causes of death (non-communicable chronic diseases, other communicable diseases and injuries) follows the global burden of disease (GBD) approach that uses a parsimonious regression technique to related mortality rates of 10 major disease clusters with GDP, smoking behaviour and human capital ([[Mathers and Loncar, 2006]]). This methodology is used for the causes of death related to urban air pollution. | The risk-factor-attributable component is based on a multi-state approach, distinguishing exposure, disease and death ([[WHO, 2002]];[[Cairncross and Valdmanis, 2006]]). This implies that for various health-risk factors, incidence and case fatality rates (i.e. the ratio of the number of deaths caused by a specific disease over the number of diagnosed cases) are taken into account. The level of health services modifies case fatality rates. This methodology is used for malaria, diarrhoea and pneumonia; the approach for protein deficiency is discussed below. The method for projecting mortality due to other causes of death (non-communicable chronic diseases, other communicable diseases and injuries) follows the global burden of disease ([[HasAcronym::GBD]]) approach that uses a parsimonious regression technique to related mortality rates of 10 major disease clusters with GDP, smoking behaviour and human capital ([[Mathers and Loncar, 2006]]). This methodology is used for the causes of death related to urban air pollution. | ||
The GISMO health model considers mortality due to (i) malaria; (ii) communicable and infectious diseases associated with undernourishment, poor access to safe drinking water and basic sanitation and poor indoor air quality; (iii) diseases caused by poor outdoor air quality; (iv) HIV-AIDS; and (v) chronic diseases including high blood pressure and obesity. Here, we only discuss the first three causes of mortality as they are linked to environmental factors. The mortality rate due to a specific disease is a multiplication of the incidence rate (fraction of the population with the specific disease) and the case fatality rate (the fraction of people who die from a specific disease), distinguishing for the two sexes and five-year age cohorts. These mortality rates can then be used to calculated age-specific life expectancy (for details see [[Hilderink, 2000]]). | The GISMO health model considers mortality due to (i) malaria; (ii) communicable and infectious diseases associated with undernourishment, poor access to safe drinking water and basic sanitation and poor indoor air quality; (iii) diseases caused by poor outdoor air quality; (iv) HIV-AIDS; and (v) chronic diseases including high blood pressure and obesity. Here, we only discuss the first three causes of mortality as they are linked to environmental factors. The mortality rate due to a specific disease is a multiplication of the incidence rate (fraction of the population with the specific disease) and the case fatality rate (the fraction of people who die from a specific disease), distinguishing for the two sexes and five-year age cohorts. These mortality rates can then be used to calculated age-specific life expectancy (for details see [[Hilderink, 2000]]). | ||
(i) Malaria risk. In GISMO, incidence rates of malaria are determined by the areas which are suitable for the malaria mosquito, based on the monthly climatic factors of temperature and precipitation ([[Craig et al., 1999]]). Incidence rates are decreased by the level of insecticide treated bed nets and indoor residual spraying, modelled separately as potential policy options. The case fatality rate of malaria is increased by underweight levels and decreased by case management, i.e. treatment. | (i) Malaria risk. In the [[GISMO model]], incidence rates of malaria are determined by the areas which are suitable for the malaria mosquito, based on the monthly climatic factors of temperature and precipitation ([[Craig et al., 1999]]). Incidence rates are decreased by the level of insecticide treated bed nets and indoor residual spraying, modelled separately as potential policy options. The case fatality rate of malaria is increased by underweight levels and decreased by case management, i.e. treatment. | ||
(ii) Access to food, water and energy. GISMO relates incidence and case fatality rates of major communicable (infectious) diseases to access to food, water and energy (see Table), with access defined by per-capita food availability, access to safe drinking water and improved sanitation, and access to modern energy sources for cooking and heating. The per-capita food availability (Kcal/cap/day) is obtained from the | (ii) Access to food, water and energy. GISMO relates incidence and case fatality rates of major communicable (infectious) diseases to access to food, water and energy (see Table), with access defined by per-capita food availability, access to safe drinking water and improved sanitation, and access to modern energy sources for cooking and heating. The per-capita food availability (Kcal/cap/day) is obtained from the [[Agricultural economy and forestry]] module. The levels of access to safe drinking water and improved sanitation are modelled separately by applying linear regression. The explanatory variables include GDP per capita, urbanisation rate and population density. Developments in water supply are assumed to be implemented ahead of sanitation. As such, developments in access follow a pathway from no sustainable access to safe drinking water and basic sanitation, to improved water supply only, improved water supply and sanitation, household connection for water supply only, and to a household connection for watersupply and sanitation. The level of access to modern energy sources for cooking and heating distinguishes between the use of 1) traditional biomass and coal on traditional stoves; 2) traditional biomass and coal on improved stoves; and 3) the use of modern energy carriers (electricity, natural gas, LPG, kerosene, modern biofuels and decentralised renewable sources). Trends in access to modern energy sources are taken from the TIMER residential [[Energy demand]] model. | ||
{{FigureTemplate|Table_HD.png}} | {{FigureTemplate|Table_HD.png}} | ||
| Line 21: | Line 21: | ||
Child underweight and prevalence of undernourishment. For children under the age of five, undernourishment is expressed as underweight (measured as weight-for-age), whereas for older ages prevalence of undernourishment is used. The direct effect of undernourishment is protein deficiency, which for children mortality rates is scaled to their underweight status; for older age groups, mortality rates are scaled to levels of undernourishment. Indirectly, undernourishment increases the incidence of diarrhoea and pneumonia, and the case fatality of malaria, diarrhoea and pneumonia. These indirect effects are only modelled for children under the age of five. | Child underweight and prevalence of undernourishment. For children under the age of five, undernourishment is expressed as underweight (measured as weight-for-age), whereas for older ages prevalence of undernourishment is used. The direct effect of undernourishment is protein deficiency, which for children mortality rates is scaled to their underweight status; for older age groups, mortality rates are scaled to levels of undernourishment. Indirectly, undernourishment increases the incidence of diarrhoea and pneumonia, and the case fatality of malaria, diarrhoea and pneumonia. These indirect effects are only modelled for children under the age of five. | ||
Child underweight as a result of chronic undernourishment is modelled as a function of improvements in average food intake, the ratio of female to male life expectancy at birth, female enrolment in secondary education and access to clean drinking water (Smith and Haddad 2000). Based on a normal distribution, the total number of underweight children is divided into three groups of mild, moderate and severe underweight (De Onis and Blossner 2003). | Child underweight as a result of chronic undernourishment is modelled as a function of improvements in average food intake, the ratio of female to male life expectancy at birth, female enrolment in secondary education and access to clean drinking water ([[Smith and Haddad, 2000]]). Based on a normal distribution, the total number of underweight children is divided into three groups of mild, moderate and severe underweight ([[De Onis and Blossner, 2003]]). | ||
The prevalence of undernourishment is calculated from per-capita food availability and the minimum energy requirements from FAO (FAO 2003). The calculations use a lognormal distribution function determined by mean food consumption and a coefficient of variation. The coefficient of variation decreases over time as a function of per-capita GDP. Finally, the minimum dietary energy requirement is derived by aggregating region-specific sex-age energy requirements weighted by the proportion of each sex and age group in the total population, including a so-called pregnancy allowance. | The prevalence of undernourishment is calculated from per-capita food availability and the minimum energy requirements from FAO ([[FAO, 2003]]). The calculations use a lognormal distribution function determined by mean food consumption and a coefficient of variation. The coefficient of variation decreases over time as a function of per-capita GDP. Finally, the minimum dietary energy requirement is derived by aggregating region-specific sex-age energy requirements weighted by the proportion of each sex and age group in the total population, including a so-called pregnancy allowance. | ||
Incidence rates of pneumonia, chronic obstructive pulmonary disease (COPD) and lung cancer are increased by indoor air pollution caused by cooking and heating with traditional biomass and coal. | Incidence rates of pneumonia, chronic obstructive pulmonary disease ([[HasAcronym::COPD]]) and lung cancer are increased by indoor air pollution caused by cooking and heating with traditional biomass and coal. | ||
Simultaneously, incidence rates and case fatality rates are increased by child underweight levels. | Simultaneously, incidence rates and case fatality rates are increased by child underweight levels. | ||
Incidence rates of diarrhoea depend on the different levels of access to drinking water and sanitation facilities, child underweight levels and also on climate change. Case fatality rates are increased by underweight levels and decreased by the level of oral rehydration therapy. | Incidence rates of diarrhoea depend on the different levels of access to drinking water and sanitation facilities, child underweight levels and also on climate change. Case fatality rates are increased by underweight levels and decreased by the level of oral rehydration therapy. | ||
(iii) Mortality associated with urban air pollution. Mortality rates of lung cancer, cardiopulmonary diseases and acute respiratory infections due to urban air pollution (i.e. PM10 and PM2.5 concentration levels) are derived by applying the GBD methodology (Mathers and Loncar 2006). Based on the emissions of NOx, SO2 and black carbon ( | (iii) Mortality associated with urban air pollution. Mortality rates of lung cancer, cardiopulmonary diseases and acute respiratory infections due to urban air pollution (i.e. PM10 and PM2.5 concentration levels) are derived by applying the GBD methodology ([[Mathers and Loncar, 2006]]). Based on the emissions of NOx, SO2 and black carbon ([[Emissions]]), PM10 concentration levels are determined using the Global Urban Air quality Model (GUAM). GUAM originates from the GMAPS model ([[Pandey et al., 2006]]), which determines PM10 concentration levels by economic activity, population, urbanisation and meteorological factors. PM2.5 concentrations are obtained using a region-specific PM10–PM2.5 ratio. Based on these concentration levels and the exposed population, mortality attributable to the aforementioned causes of death is derived using relative risks. These relative risks have been obtained from epidemiological literature ([[Dockery et al., 1993]]; [[Pope et al., 1995]]). | ||
== GISMO poverty model == | == GISMO poverty model == | ||
In general, people are considered poor if their consumption or income levels fall below the level that is necessary to meet their basic needs, the ‘poverty line’. The poverty headcount (people living below the poverty line) is conducted by applying a log-normal distribution using per-capita income and a GINI coefficient to describe its distribution over a population. The poverty module addresses people living below the international poverty lines of USD 1.25 and USD 2 per day, at 2005 PPP, as defined by the World Bank (Ravallion et al. 2008). | In general, people are considered poor if their consumption or income levels fall below the level that is necessary to meet their basic needs, the ‘poverty line’. The poverty headcount (people living below the poverty line) is conducted by applying a log-normal distribution using per-capita income and a GINI coefficient to describe its distribution over a population. The poverty module addresses people living below the international poverty lines of USD 1.25 and USD 2 per day, at 2005 PPP, as defined by the World Bank ([[Ravallion et al., 2008]]). | ||
== GISMO education model == | == GISMO education model == | ||
The education model addresses future developments in school enrolment and educational attainment, including literacy rates, for three levels of education: primary, secondary and tertiary. The model tracks the shares of the highest completed education and the average years of schooling per cohort. The enrolment ratios per educational level are determined, using cross-sectional relationships with per-capita GDP (PPP). The ages at which children attain a certain educational level are assumed to be equal across all regions. Literacy rates are simulated by the share of the population aged 15+, who have completed at least their primary education. Furthermore, to take account of autonomous increases in literacy levels, those of the population between the ages of 15 and 65 are increase by 0.3%, annually. | The education model addresses future developments in school enrolment and educational attainment, including literacy rates, for three levels of education: primary, secondary and tertiary. The model tracks the shares of the highest completed education and the average years of schooling per cohort. The enrolment ratios per educational level are determined, using cross-sectional relationships with per-capita GDP (PPP). The ages at which children attain a certain educational level are assumed to be equal across all regions. Literacy rates are simulated by the share of the population aged 15+, who have completed at least their primary education. Furthermore, to take account of autonomous increases in literacy levels, those of the population between the ages of 15 and 65 are increase by 0.3%, annually. | ||
}} | }} | ||
Revision as of 13:05, 9 December 2013
Parts of Human development/Description
| Component is implemented in: |
|
| Related IMAGE components |
| Projects/Applications |
| Models/Databases |
| Key publications |
| References |
{kind=link}