Human development/Description: Difference between revisions
Jump to navigation
Jump to search
No edit summary |
No edit summary |
||
| Line 1: | Line 1: | ||
{{ComponentDescriptionTemplate | {{ComponentDescriptionTemplate | ||
|Status=On hold | |Status=On hold | ||
|Reference=Hilderink, 2000; UNDP, 1990; UNDP, 2010; WHO, 2002; Cairncross and Valdmanis, 2006; Mathers and Loncar, 2006; Craig et al., 1999; Smith and Haddad, 2000; De Onis and Blossner, 2003; FAO, 2003; Mathers and Loncar, 2006; Pandey et al., 2006; Dockery et al., 1993; Pope et al., 1995; Ravallion et al., 2008; | |Reference=Hilderink, 2000; UNDP, 1990; UNDP, 2010; WHO, 2002; Cairncross and Valdmanis, 2006; Mathers and Loncar, 2006; Craig et al., 1999; Smith and Haddad, 2000; De Onis and Blossner, 2003; FAO, 2003; Mathers and Loncar, 2006; Pandey et al., 2006; Dockery et al., 1993; Pope et al., 1995; Ravallion et al., 2008; | ||
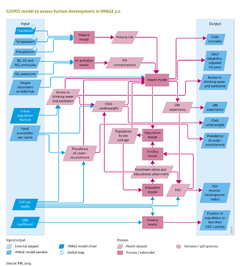
|Description=In the GISMO model, the impacts of global environmental change on human development are modelled by considering impacts on human health – either directly, for example, via the impact of climate change on malaria, or indirectly, such as by the impact of climate change on food availability. In addition to environmental factors, human health is also driven by socioeconomic factors, including income levels and educational attainment. To take account of these different factors and their interrelation, the GISMO model consists of three modules that address human health, poverty and education (see Figure on the right). The modules are linked through a cohort component population model, including endogenous fertility and mortality (for details see [[Hilderink, 2000]]). Fertility levels are modelled using a convergence level that is determined by female educational levels, and a speed of convergence, determined by the human development index (HDI) (see below). Mortality rates are determined by the health module, which is discussed in further detail in the remainder of this section. Future trends in migration, including urbanisation, are put exogenously into the model (for details see [[Hilderink, 2000]]) | |Description=In the GISMO model, the impacts of global environmental change on human development are modelled by considering impacts on human health – either directly, for example, via the impact of climate change on malaria, or indirectly, such as by the impact of climate change on food availability. In addition to environmental factors, human health is also driven by socioeconomic factors, including income levels and educational attainment. To take account of these different factors and their interrelation, the GISMO model consists of three modules that address human health, poverty and education (see Figure on the right). The modules are linked through a cohort component population model, including endogenous fertility and mortality (for details see [[Hilderink, 2000]]). Fertility levels are modelled using a convergence level that is determined by female educational levels, and a speed of convergence, determined by the human development index (HDI) (see below). Mortality rates are determined by the health module, which is discussed in further detail in the remainder of this section. Future trends in migration, including urbanisation, are put exogenously into the model (for details see [[Hilderink, 2000]]) | ||
| Line 30: | Line 30: | ||
Incidence rates of diarrhoea depend on the different levels of access to drinking water and sanitation facilities, child underweight levels and also on climate change. Case fatality rates are increased by underweight levels and decreased by the level of oral rehydration therapy. | Incidence rates of diarrhoea depend on the different levels of access to drinking water and sanitation facilities, child underweight levels and also on climate change. Case fatality rates are increased by underweight levels and decreased by the level of oral rehydration therapy. | ||
(iii) Mortality associated with urban air pollution. Mortality rates of lung cancer, cardiopulmonary diseases and acute respiratory infections due to urban air pollution (i.e. PM10 and PM2.5 concentration levels) are derived by applying the GBD methodology ([[Mathers and Loncar, 2006]]). Based on the emissions of NOx, SO2 and black carbon ([[Emissions]]), PM10 concentration levels are determined using the Global Urban Air quality Model (GUAM). GUAM originates from the GMAPS model ([[Pandey et al., 2006]]), which determines PM10 concentration levels by economic activity, population, urbanisation and meteorological factors. PM2.5 concentrations are obtained using a region-specific PM10–PM2.5 ratio. Based on these concentration levels and the exposed population, mortality attributable to the aforementioned causes of death is derived using relative risks. These relative risks have been obtained from epidemiological literature ([[Dockery et al., 1993]]; [[Pope et al., 1995]]). | (iii) Mortality associated with urban air pollution. Mortality rates of lung cancer, cardiopulmonary diseases and acute respiratory infections due to urban air pollution (i.e. PM10 and PM2.5 concentration levels) are derived by applying the GBD methodology ([[Mathers and Loncar, 2006]]). Based on the emissions of NOx, SO2 and black carbon ([[Emissions]]), PM10 concentration levels are determined using the [[Global Urban Air quality Model]] (GUAM). GUAM originates from the GMAPS model ([[Pandey et al., 2006]]), which determines PM10 concentration levels by economic activity, population, urbanisation and meteorological factors. PM2.5 concentrations are obtained using a region-specific PM10–PM2.5 ratio. Based on these concentration levels and the exposed population, mortality attributable to the aforementioned causes of death is derived using relative risks. These relative risks have been obtained from epidemiological literature ([[Dockery et al., 1993]]; [[Pope et al., 1995]]). | ||
== GISMO poverty model == | == GISMO poverty model == | ||
Revision as of 13:52, 9 December 2013
Parts of Human development/Description
| Component is implemented in: |
|
| Related IMAGE components |
| Projects/Applications |
| Models/Databases |
| Key publications |
| References |
{kind=link}